 How can I boost my fertility?Getting pregnant isn’t easy, but there are things you (and your partner) can do to boost your fertility and your chances of conceiving each cycle? Having regular intercourse will certainly help, but there are a variety of other ways to help your body get to its most fertile state.
Total healthYour general health and fertility health are more closely related than you might think: fertility is just one component of your total body health, after all. Increase your chances of conceiving and prepare your body for a healthy pregnancy by keeping your general health strong. Be sure to get enough sleep, stay active, and maintain a healthy diet. Sleep Your body rebuilds and recovers while you’re sleeping, so getting enough rest is very important to maintain the timing of your menstrual cycle. In addition, your body produces the hormone leptin while you are asleep. Leptin helps regulate your cycle and ensure that you ovulate and menstruate. Getting enough sleep will also help to prevent or manage stress, which can seriously hamper fertility. Ovia starts you out with a sleep goal of 8 hours each night. Activity Another key piece of your general health is physical activity. Staying active is important for keeping your body strong (which you’ll need when you’re supporting a baby during pregnancy) and managing your weight. Regular exercise can help you manage stress, which can often affect your cycle. Women who are trying to conceive should make sure to stay active, whether that’s by walking, lifting weights, doing yoga, or anything else. We recommend getting at least 30 minutes of activity each day. Nutrition The human body is a well-oiled machine, and like all machines, it needs the highest-quality fuel possible to run at its best. Processed and fried foods, alcohol, and low-fat dairy products, among others, can have a considerable negative effect on your fertility. You need lots of folate, Vitamin C, and other healthy nutrients to keep your ovulation as regular as possible. Keeping to a diet high in fruits, leafy greens, and lean proteins (salmon, eggs, chicken, etc.) is sure to get your body as fertile as possible and prepare you for pregnancy. Weight Having both too high and too low a weight has a considerable effect on fertility. Women who are overweight may notice irregular ovulations and are more likely to experience the condition of infertility known as Polycystic Ovarian Syndrome (PCOS). Those who are significantly underweight also face a more difficult road to pregnancy, as it can seriously affect your hormonal balance and cycle regularity. Getting and keeping yourself at a healthy weight with the help of proper sleep, activity, and nutrition is a great way to help boost your fertility and chances of conceiving. Both partners matter! In cases of infertility, both partners are often equally likely to contribute to difficulties conceiving. For example, approximately ⅓ of cases of infertility affect the woman only, while ⅓ affect the man only, and the other ⅓ have unknown causes. The very same things that can help or harm your fertility can also affect your partner’s. On the negative side, being overweight or overly stressed, smoking and drinking alcohol, and using drugs can hurt fertility; on the positive side, getting proper sleep, activity, and nutrition can boost fertility. Getting pregnant is a game for two, so it’s important that both you and your partner keep yourselves as healthy and fit as possible as you try to conceive. Keeping your general health strong is a vital but often overlooked part of conceiving. All of the sex positions, oil-based lubricants, and fertility dances in the world won’t help you get pregnant if your general health is not where it should be. Read moreSources
0 Comments
 Don’t panic! It’s going to be OK. Your baby is breech for a reason. (S)he may or may not turn and can do so even right before birth. So, be patient.
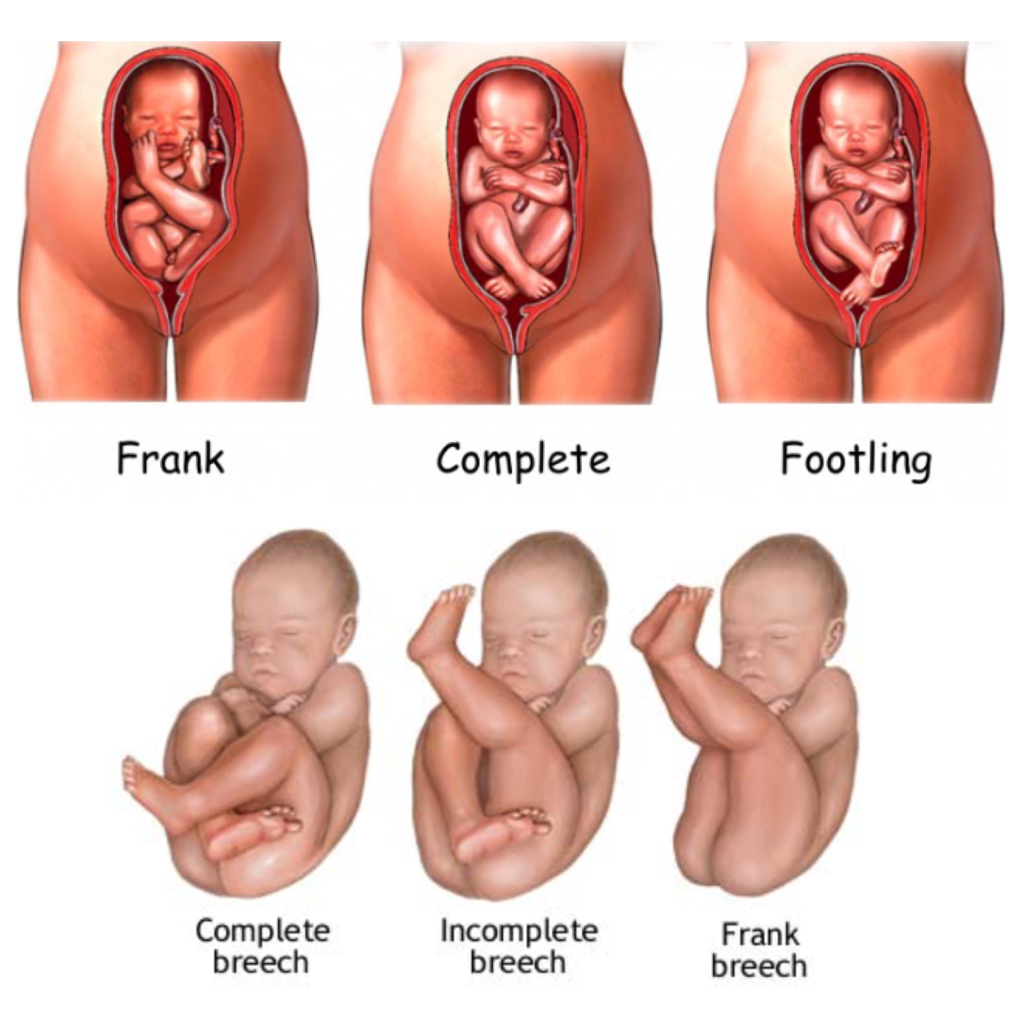
Which breech presentation is your baby favoring? There are three common types. Frank Breech, which tends to be the most favorable. This is when baby’s bottom presents first and feet are by the head. Footling Breech is when baby has one or both feet presenting first. Complete Breech is when your baby is comfy sitting cross legged. There are things you can do to help baby turn if that is what baby wants. Remember, your baby knows best what position to be in for his/her birth. Look into the following options: •Chiropractic adjustments •Acupuncture •Spinning babies •Moxibustion •Playing music low on the belly and placing frozen peas on top of your belly. Fun things that won’t hurt any, so why not try? •Visualize, meditate and pray (this is more powerful than most people realize). •Hire a care provider who is comfortable and knows what to do (and not to do) for breech births. •Acceptance and Faith (your baby knows exactly what (s)he is doing). Even when you decide to have faith in your body and your baby, you still want to be prepared and know how to help him/her gently enter this world. Here are some things to consider and research. Know and be firm in your knowledge that a breech baby does not automatically mean c-section. Make sure your OB or midwife is 100% on board and does not fear breech birth. Always listen to YOUR intuition. If you have a fear, process it. If someone else does, don’t waiver in your faith. Trust your gut! When birthing, get in a favorable position like standing, squatting, or even hand and knees (unless your body is telling you different). Read a lot of great breech birth stories! I've posted here some awesome pictures for your viewing above to help you understand. Do NOT let anyone (your midwife, spouse, doula, OB, etc.) pull on baby! Something to educate yourself on further is making sure baby’s head is birthed before they start breathing. The book Emergency Childbirth by Gregory J. White was helpful for me. Have a back up plan. There is nothing wrong with having one. Don’t focus on it, but know it’s there. Continue to have faith that your vaginal birth will be wonderful and successful. If you get nothing else from this post, remember this: Even IF you have a c-section, WAIT. Wait for baby to start labor. I say this for two reasons. First, you will know for sure that your baby is ready to be earthside. Second, is that you have given your baby every chance to turn head down. In hindsight, my first baby was born at least 3 weeks early as all my others. A baby that is breech is not an automatic dangerous situation or cesarean. Breech babies have different risk factors and those should be discussed with your care provider, so you CAN make an informed decision on what is best for your baby and birth, with their support. -Natasha  With many hospitals and private obstetricians requiring you to book pretty much as soon as a pregnancy is confirmed, the temptation is strong to just get into whoever you can and be grateful you got in to anyone at all. After all, caregivers are all pretty much the same, aren’t they?
Well…actually, no. There are some key differences between midwifery and obstetric models of care. Just as no two accountants or lawyers practice in the same way, maternity care givers are also a diverse bunch. Amongst other things the way they care for women in pregnancy and labour is influenced by their training, their own previous experiences, and their hard wired beliefs around birth. This means its generally a good idea to talk with a few in early pregnancy, and make an effort to find a care provider whose approach aligns with yours. This list is focused on specific, key questions that will help you identify a care giver who is genuinely supportive of natural birth – but it’s by no means comprehensive! If you’re looking for this type of care, it’s helpful to understand what a potential care provider views as a “hands off” situation, and when they believe intervention might be needed. These questions should give you a feel for where your midwife or obstetrician stands, and can be a jumping off point for exploring your own feelings about intervention in your birth as well. 1. What’s your approach to post dates pregnancies? At what point would the care giver recommend you consider induction or other intervention to start labour? In Queensland, 24% of women will be induced, and a further 19% will have their labour augmented (ie. be given an intravenous drug during labour to regulate or strengthen contractions). Most commonly, inductions are scheduled when a pregnancy lasts beyond the estimated due date. Caregivers will vary as to how far is too far for them – anything from a couple of days, to a few weeks. If you’d like to avoid induction where possible, finding a care giver with a more relaxed approach can mean you and your baby navigate the final days of your pregnancy without pressure. 2. What’s your caesarean rate for normal, uncomplicated pregnancies? If a prospective care provider is evasive or vague on this question it may be a red flag. Our caesarean rate in Australia averages around 30%. While private hospitals don’t have to publish their data on an individual level, as a group they consistently report rates above this. Asking about the rate for uncomplicated pregnancies removes any confusion that may be caused by the inclusion of high risk pregnancies (these would usually be attended by obstetricians). 3. What’s your approach to the management of gestational diabetes? Gestational diabetes is being diagnosed more frequently in women with no prior risk factors, and in recent years the cut off point for diagnosis has been dropping. Around 8% of pregnant women will be diagnosed with gestational diabetes, most around the 28th week of pregnancy. If you’re one of them, the way your care provider routinely manages a GD diagnosis can have major implications for your pregnancy and labour. 4. Under what circumstances, if any, would you be likely to perform an episiotomy? Fortunately episiotomy rates are declining, but they’re still unacceptably high, especially among first time mothers. A care provider with a high episiotomy rate may be one who is quick to intervene generally. If this is your first baby, you could ask how many first time mothers in their hospital or practice receive an episiotomy to get a clearer picture. 5. What will happen if my baby is breech at term? This is a loaded question and the answer will tell you quite a bit! It’s highly unlikely that your baby will be breech at term, but asking your care provider what they’d usually do in this situation can be enlightening. Obstetricians and midwives who don’t view breech position alone as an automatic indication for caesarean are very likely to be a low intervention, hands off care provider for a woman with a head down baby. 6. When would you recommend routine continuous monitoring of my baby in labour? Continuous monitoring during spontaneous, normal labour in low risk women has been shown to increase the likelihood of caesarean without improving outcomes for babies. If your pregnancy has been normal and you labour spontaneously and unmedicated, intermittent listening with a doppler has been shown to be as safe – and won’t increase your risk of surgery. Nonetheless, some care providers insist on continuous monitoring for all women, regardless of their risk status. If you want to use the shower for pain relief and be able to move around to manage pain, this might be something to ask about. Depending on your priorities for your own birth, this list barely scratches the surface of what you might need to ask a potential care provider. Can you think of anything else it would be important to know? If so, email me, I want to hear them! Natasha  Please come out and join me every second Sunday! Hope to see you there! 
Looking for a more natural approach to improving your health and wellness? Let me help you Invest in your life and longevity with Dōterra Essential oils! This is a true STEAL!!! Get it while supplies last @ http://mydoterra.com/doterradoula or contact me directly today to set up an educational class.

|
Archives
November 2016
Categories |
 RSS Feed
RSS Feed